Abstract
Infection Prevention and Control (IPC) standard protocols are not just administrative tasks, they are essential, life-saving skills. The study determined the competency level on Infection Prevention and Control IPC standard protocols among emergency and operating room nurses in the 5th District of Camarines Sur. Specifically, it sought answers to the demographic profile of the respondents and the level of competency along hand hygiene, use of Personal Protective Equipment PPE, and prevention of needle stick and sharp injuries. The study utilized the descriptive-correlational method using a questionnaire checklist as the data-gathering instrument. The respondents of the study were 70 emergency and operating room nurses from the selected hospitals in Rinconada, and the total enumeration method was utilized. Findings showed that most were 25 years old and below (23 or 32.86 percent). The majority were males (50 or 71.43 percent). In terms of training and seminars attended related to IPC, majority of the respondents reported non-attendance (59 or 84.28 percent). The competency level on infection prevention and control standard protocols revealed that the respondents were very high competent in hand hygiene with an AWM of 4.68, very high competent in the use of PPE with an AWM of 4.42, and high competent in the prevention of needle stick and sharp injuries with an AWM of 4.19. Statistical tests showed that educational attainment, area of assignment, length of service, and relevant trainings attended had a significant relationship with the level of competency. It is recommended that the proposed training program titled "Enhancing Infection Prevention and Control Competencies among Emergency and Operating Room Nurses in the 5th District of Camarines Sur" may be formally adopted and implemented by the hospital management. Regular evaluation and continuous refinement of the program based on staff feedback and clinical outcomes may also be established to ensure it effective and sustainable occupational safety and quality patient care.
Keywords
Competency Infection Prevention and Control Standards Protocols Emergency and Operating Room Nurses.
Introduction
Globally, the impact of HAIs continues to be a significant challenge, especially in the high-pressure and unpredictable settings of the Emergency Room (ER) and Operating Room (OR). The World Health Organization (2026) consistently stress that although IPC policies are internationally well documented, nurse competency and compliance with these policies vary considerably, depending on environmental stressors, staffing, and the dynamic nature of emergency care. A recent global assessment shows that while nurses have a high level of awareness of the risk of infection, their competency needs ongoing specific training to ensure that knowledge is applied in practice (Kim & Kang, 2025).
Zooming into the national perspective, the Philippines faces its own distinct set of challenges in maintaining stringent IPC standards amid varying levels of healthcare resource availability. The DOH strictly mandates IPC measures to counteract the escalating risk of HAIs across the country. This is legally anchored in DOH Administrative Order No. 2022-0051, the Revised National Policy on Infection Prevention and Control in All Public and Private Health Facilities, which mandates all healthcare facilities to establish comprehensive IPC programs with written guidelines on hand hygiene, standard precautions, aseptic techniques, and environmental cleaning. Furthermore, Republic Act No. 11223, known as the Universal Health Care Act, which guarantees all Filipinos access to quality healthcare services while protecting them from health risks.
A recent Philippine-based study underscores the urgency of addressing these IPC competencies among nurses. Research conducted in a tertiary hospital in Baguio City evaluated the knowledge and practices of nurses regarding HAIs, revealing that while foundational knowledge is present, actual clinical adherence is heavily influenced by organizational support, working conditions, and regular performance feedback (Campo & Remon, 2025).
In the Bicol Region, particularly the province of Camarines Sur, DOH Bicol has actively promoted infection prevention and control practices through its Center for Health Development, emphasizing collaborative efforts among healthcare facilities to ensure patient safety. The Bicol Medical Center in Camarines Sur has established dedicated IPC units and has received assessments from DOH Bicol's Health Facility Development Unit, demonstrating the region's commitment to strengthening IPC programs.
Infection Prevention and Control (IPC) is the silent defender of the heart and soul of the healthcare profession. This is more than a set of clinical practices; it reflects an unwavering commitment to the ethical imperative of preserving hospitals as a place of healing, not harm. For healthcare workers, especially frontline professionals, IPC standard protocols are not just administrative tasks, they are essential, life-saving skills. It is the ultimate safeguard against the insidious threat of healthcare-associated infections (HAIs), safeguarding not only the vulnerable patients entrusted to the care of clinicians but also the unsung heroes of health care who place their own health at risk to care for others.
This critical need for strong IPC practices is in line with the United Nations Sustainable Development Goal (SDG) 3, which aims to ensure healthy lives and promote well-being for all ages. Good IPC practice is crucial to the attainment of target 3.8, which relates to universal health coverage and accessible and quality essential health-care services, and target 3.D, which focuses on strengthening capacity for early warning, risk reduction and management of national and global health risks. Competent emergency and operating room nurses are integral in strengthening robust health systems to support and fulfil these global health goals (United Nations, 2026).
Driven by these global, national, and local imperatives, this study aims to comprehensively assess the competency level on IPC standard protocols among emergency and operating room nurses in 5th District of Camarines Sur. Specifically, the research seeks to determine their current knowledge and actual clinical practices.
Methodology
The research utilizes a descriptive-correlational method to examine the relationship between the demographic profiles of nursing personnel and their competency levels regarding infection prevention and control (IPC) protocols. The study was conducted within the 5th District of Camarines Sur, specifically five private healthcare institutions: Sta. Maria Josefa Hospital Foundation, Inc., CHMSC Lourdes Hospital, Our Lady Mediatrix Hospital, VTMGHI, and the Medical Mission Group Hospital. Using purposive sampling and total enumeration, the researcher identified 70 emergency and operating room nurses as the primary respondents based on their direct involvement in high-stakes infection control environments.
Data collection is facilitated through a self-made, two-part questionnaire checklist that underwent a rigorous validation process, including expert evaluation for face and content validity and a pilot test with 10 staff nurses. Part I of the instrument establishes the demographic profile of the nurses, while Part II assesses IPC competency in areas such as hand hygiene, the use of personal protective equipment (PPE), and the prevention of needle stick injuries. The questionnaires were distributed and retrieved manually to maintain anonymity and ensure that the process did not interfere with hospital operations or patient care duties.
For the statistical treatment of data, the researcher employs percentages, rankings, and frequencies to describe the demographic characteristics of the sample. A weighted mean is calculated using a five-point Likert scale to quantify competency levels, ranging from "Not at all Competent" to "Very Highly Competent". Additionally, the Chi-square test is utilized to test the null hypothesis and determine if there are significant associations between the nurses' demographic variables and their adherence to IPC standard protocols.
Results and Discussion
Demographic Profile
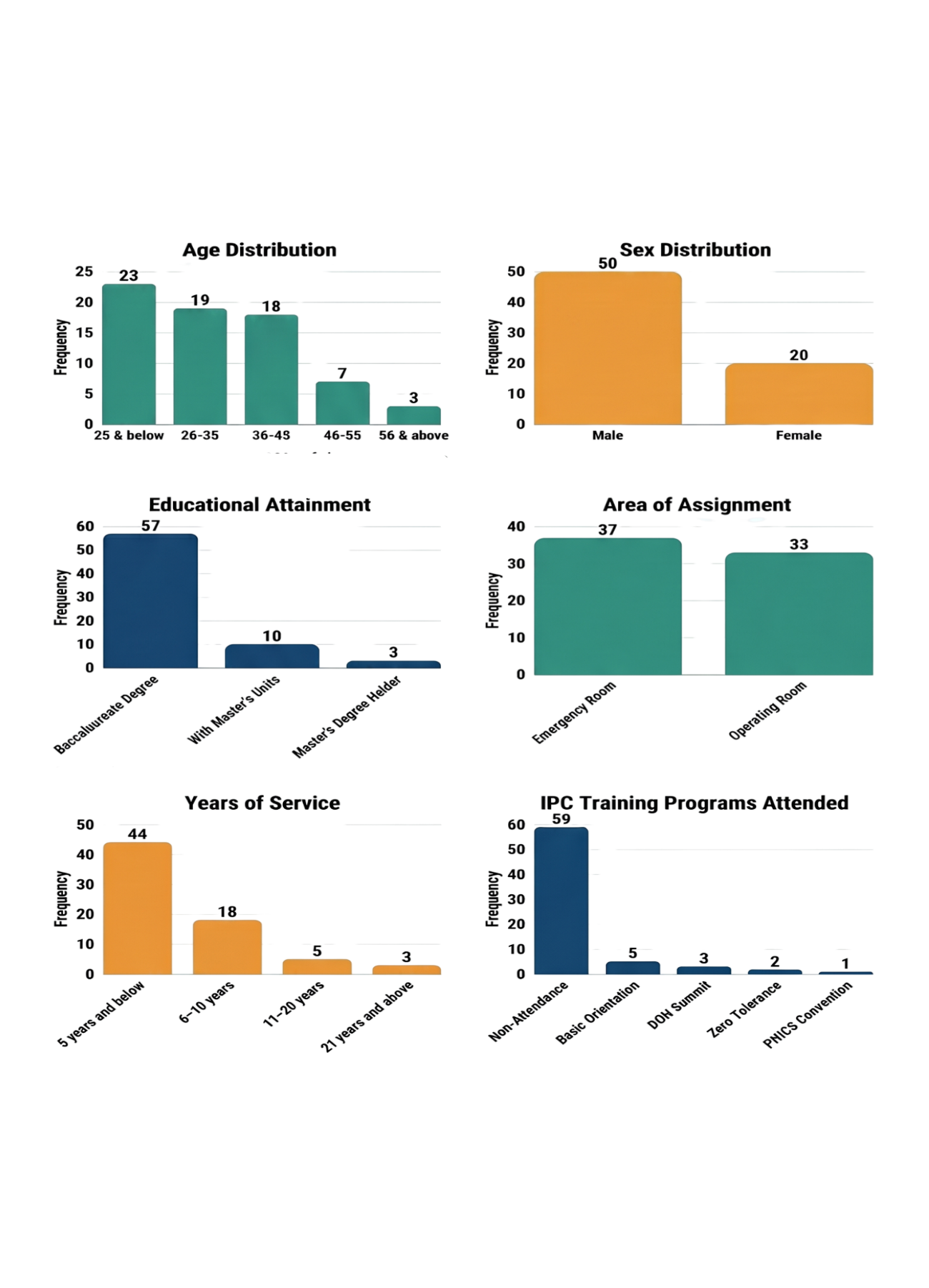
As presented in Figure 1, the demographic profile shows that the 70 emergency and operating room nurses are distributed across a wide age range, with the largest group aged 25 years and below (23, 32.86%), followed by those aged 26–35 years (19, 27.14%), 36–45 years (18, 25.71%), 46–55 years (7, 10%), and 56 years and above (3, 4.29%). In terms of sex, the sample is predominantly male, with 50 nurses (71.43%) compared to 20 females (28.57%). With respect to educational attainment, most respondents hold a baccalaureate degree (57, 81.43%), while 10 (14.29%) have earned master’s units and 3 (4.28%) have completed a master’s degree, indicating that the majority possess basic professional qualifications, with a smaller proportion pursuing or having achieved graduate-level education.
Work-related profile further show that 37 nurses (52.86%) are assigned to the Emergency Room and 33 (47.14%) to the Operating Room, reflecting a nearbalanced distribution between these two critical care areas. The majority have relatively short professional tenure, with 44 (62.86%) having been in service for 5 years and below, 18 (25.71%) with 6–10 years, 5 (7.14%) with 11–20 years, and 3 (4.29%) with 21 years and above, indicating a largely earlycareer workforce. In terms of IPC training/seminar, 59 respondents (84.28%) reported no attendance in any IPCrelated training, while only a small proportion had participated in programs such as Basic Infection Prevention and Control Orientation (5, 7.14%), the DOH National Infection Prevention and Control Summit (4.29%), Zero Tolerance: Essentials of IPC (2.86%), and the PHICS Annual Convention (1.43%), underscoring a substantial gap in formal IPC training exposure among the respondents.
Figure: Demographic Profile
Competency Level on Infection Prevention and Control Standard Protocols
Hand hygiene. The data presented in Table 1 present the level of competency on Infection Prevention and Control standard protocols along hand hygiene among emergency and operating room nurses. With an AWM of 4.68, interpretated as very highly competent. Among the indicators, cleaning hands before eating ranked highest with a WM = 4.79, very high competent, followed by cleaning hands before a clean or aseptic procedure and cleaning hands after touching contaminated items or surfaces, both of which shared a WM = 4.74, very highly competent. Conversely, cleaning hands after using the restroom (WM = 4.67, very highly competent), followed by cleaning before and after touching surgical instruments or equipment and cleaning hands before touching a patient or their environment, both of which ranked the lowest at WM = 4.51, very highly competent. This pattern indicated that nurses consistently practiced exceptional adherence during explicit contamination risks and self-protection scenarios but showed a relative decrease in competency during routine patient contact and equipment handling.
| Table 1 : Competency Level on Infection Prevention and Control standard protocols along Hand Hygiene | ||
| Indicators | Weighted Mean | Verbal Interpretation |
| Clean hands before eating. | 4.79 | Very Highly Competent |
| Clean hands before a clean or aseptic procedure. | 4.74 | Very Highly Competent |
| Clean hands after touching contaminated items or surfaces. | 4.74 | Very Highly Competent |
| Clean hands when hands are visibly soiled. | 4.73 | Very Highly Competent |
| Ensure that hand hygiene products, like soap, water, and hand sanitizer, are readily available at the point of care. | 4.73 | Very Highly Competent |
| Clean hands after touching a patient or their environment, even if gloves are worn. | 4.71 | Very Highly Competent |
| Clean hands after removing gloves. | 4.70 | Very Highly Competent |
| Clean hands after using the restroom. | 4.67 | Very Highly Competent |
| Clean hands before touching a patient ortheir environment. | 4.51 | Very Highly Competent |
| Clean before and after touching surgical instruments or equipment. | 4.51 | Very Highly Competent |
| Average Weighted Mean | 4.68 | Very Highly Competent |
Use of Personal Protective Equipment (PPE). The data presented in Table 2 show the level of competency on Infection Prevention and Control standard protocols along the Use of Personal Protective Equipment (PPE) among emergency and operating room nurses. Among the indicators, shielding eyes from splashes or sprays of bodily fluids ranked highest with a WM = 4.77, very highly competent, followed by wearing gloves when handling chemicals and/or body fluids and using respiratory protection, especially during procedures involving airborne pathogens, both of which shared a WM = 4.66, very highly competent.
Conversely, wearing an apron/gown/coveralls if hazardous or infectious substances are likely to splash and attaching straps or ties around the head/neck, adjusting the flexible band to the nose bridge for a proper fit, and performing a fit-check if necessary both shared a WM = 4.17, highly competent, followed by using a respirator when hazardous or infectious substances are airborne such as tuberculosis (WM = 4.16, highly competent), and wearing hearing protection when exposed to loud noises, such as those from equipment, ranked exposures but were slightly less competent in utilizing environmental noise protection, specialized respirator fitting procedures, and situational gowning the lowest at WM=4.15, highly competent. This pattern indicated that nurses are highly proficient in routine barrier protections against direct fluid and airborne.
| Table 2: Competency Level on Infection Prevention and Control standard protocols along Use of Personal Protective Equipment (PPE) | ||
| Indicators | Weighted Mean | Verbal Interpretation |
| Shields eyes from splashes or sprays of bodily fluids. | 4.77 | Very Highly Competent |
| Wear gloves when handling chemicals and/or body fluids. | 4.66 | Very Highly Competent |
| Use respiratory protection, especially during procedures involving airborne pathogens. | 4.66 | Very Highly Competent |
| Remove PPE carefully to avoid contaminating oneself. | 4.65 | Very Highly Competent |
| Dispose of PPE in designated containers before leaving the area. | 4.64 | Very Highly Competent |
| Wear safety shoes/boots/covers if hazardous or infectious substances are likely to splash. | 4.18 | Highly Competent |
| Wear an apron/gown/coveralls-if hazardous or infectious substances are likely to splash. | 4.17 | Highly Competent |
| Attach straps or ties around the head/neck, adjust the flexible band to the nose bridge for a proper fit, and perform a fit-check if necessary. | 4.17 | Highly Competent |
| Use a respirator when hazardous or infectious substances are airborne such as tuberculosis. | 4.16 | Highly Competent |
| Wear hearing protection when exposed to loud noises, such as those from equipment. | 4.15 | Highly Competent |
| Average Weighted Mean | 4.42 | Very Highly Competent |
Prevention of needle stick and sharp injuries. The data presented in Table 3 showed the level of competency on Infection Prevention and Control standard protocols along the prevention of needle stick and sharp injuries among emergency and operating room nurses. With an AWM of 4.19, it is interpreted as highly competent. Among the indicators, handling needles and sharps with care and keeping handling to a minimum ranked highest with a WM = 4.24, very highly competent, followed by disposing of used needles in designated sharps containers immediately after use (WM = 4.23, very highly competent), and ensuring sharps. containers are clearly labeled, puncture-proof, and leak-proof (WM=4.22, very highly competent). Conversely, using the scoop-cap method to cover syringes and using devices with safety features such as safety shields or retractable needles both shared a WM=4.17, highly competent, followed by never bending, breaking, or snapping needles before disposal (WM=4.16, highly competent), and exploring the use of needleless systems with self-sealing ports and syringes ranked the lowest at WM=4.15, highly competent. This pattern indicated that nurses consistently practiced foundational sharp safety such as immediate disposal and careful handling but were slightly less competent in adopting advanced safety-engineered devices and specific behavioral prevention techniques.
| TTable 3 : Competency Level on Infection Prevention and Control standard protocols along Prevention of needle stick and sharp injuries | ||
| Indicators | Weighted Mean | Verbal Interpretation |
| Handle needlesand sharps with care and keep handling to a minimum. | 4.24 | Very Highly Competent |
| Dispose of used needles in designated sharps containers immediately after use. | 4.23 | Very Highly Competent |
| Ensure sharps containers are clearly labeled, puncture-proof, and leak-proof. | 4.22 | Very Highly Competent |
| Use devices with safety shields or retractable needles and activate safety mechanisms immediately after use. | 4.21 | Highly Competent |
| Explore needleless systems for medication administration. | 4.19 | Highly Competent |
| Avoid recapping needles by hand. | 4.18 | Highly Competent |
| Use the scoop-cap method: place the cap on a hard surface, then use one hand to hold the syringe and scoop up the cap. | 4.17 | Highly Competent |
| Use devices with safety features such as safety shields or retractable needles. | 4.17 | Highly Competent |
| Never bend, break, or snap needles before disposal. | 4.16 | Highly Competent |
| Explore the use of needleless systems with self-sealing ports and syringes | 4.15 | Highly Competent |
| Average Weighted Mean | 4.19 | Highly Competent |
Relationship between the demographic profile and Competency Level on Infection Prevention and Control standard protocols.
The data presented in Table 4 showed the relationship between the demographic profile and the competency level on Infection Prevention and Control (IPC) standard protocols along hand hygiene, use of personal protective equipment (PPE), and prevention of needle stick and sharp injuries. Across all three domains, the computed χ² values for age (computed χ² ranging from 3.28 to 4.35; critical value = 26.30, df = 16) and sex (computed χ² ranging from 1.59 to 1.77; critical value = 9.49, df = 4) fell below their respective critical values at the .05 significance level, leading to the decision to accept the null hypothesis, interpreted as not significant. Conversely, educational attainment (computed χ² = 16.18 to 16.33; critical value = 15.51, df = 8), area of assignment (computed χ²= 9.89 to 11.79; critical value = 9.49, df = 4), length of service (computed $\chi^2$ = 21.88 to 22.38; critical value = 21.03, df = 12), and relevant trainings attended (computed χ² = 27.12 to 27.15; critical value = 26.30, df = 16) yielded computed χ² values higher than their critical limits, resulting in the rejection of the null hypothesis and an interpretation of significant across all three domains.
This pattern indicated that the clinical nurses' competency in standard protocols was profoundly influenced by acquired professional variables such as higher education, specific unit assignment, cumulative clinical experience, and targeted training rather than their inherent demographic or biological profile like age and sex.
| Table 4: Relationship between the demographic profile and level of competency on Infection Prevention and Control standard protocols | ||||||
| Profile | Hand Hygiene | |||||
| df | Computed x2 | Critical x2 Value | Level of Significance | Decision | Interpretation | |
| Age | 16 | 3.47 | 26.30 | .05 | Accept Ho | Not Significant |
| Sex | 4 | 1.59 | 9.49 | .05 | Accept Ho | Not Significant |
| Educational Attainment | 8 | 16.21 | 15.51 | .05 | Reject Ho | Significant |
| Area of Assignment | 4 | 10.88 | 9.49 | .05 | Reject Ho | Significant |
| Length of Service | 12 | 22.38 | 21.03 | .05 | Reject Ho | Significant |
| Relevant Trainings Attended | 16 | 27.15 | 26.30 | .05 | Reject Ho | Significant |
| Profile | Use of Personal Protective Equipment (PPE) | |||||
| df | Computed x2 | Critical x2 Value | Level of Significance | Decision | Conclusion | |
| Age | 16 | 4.35 | 26.30 | .05 | Accept Ho | Not Significant |
| Sex | 4 | 1.63 | 9.49 | .05 | Accept Ho | Not Significant |
| Educational Attainment | 8 | 16.18 | 15.51 | .05 | Reject Ho | Significant |
| Area of Assignment | 4 | 11.79 | 9.49 | .05 | Reject Ho | Significant |
| Length of Service | 12 | 22.16 | 21.03 | .05 | Reject Ho | Significant |
| Relevant Trainings Attended | 16 | 27.14 | 26.30 | .05 | Reject Ho | Significant |
| Profile | Prevention of Needle Stick and Sharp Injury | |||||
| df | Computed x2 | Critical x2 Value | Level of Significance | Decision | Conclusion | |
| Age | 16 | 3.28 | 26.30 | .05 | Accept Ho | Not Significant |
| Sex | 4 | 1.77 | 9.49 | .05 | Accept Ho | Not Significant |
| Educational Attainment | 8 | 16.33 | 15.51 | .05 | Reject Ho | Significant |
| Area of Assignment | 4 | 9.89 | 9.49 | .05 | Reject Ho | Significant |
| Length of Service | 12 | 21.88 | 21.03 | .05 | Reject Ho | Significant |
| Relevant Trainings Attended | 16 | 27.12 | 26.30 | .05 | Reject Ho | Significant |
Conclusion
The study concludes that the respondents are predominantly young to early middleaged nurses, mostly males, baccalaureate degree holders, and largely assigned to the Emergency Room, with the majority having five years and below of nursing service and no prior training related to IPC. Within this profile, emergency and operating room nurses generally demonstrate a high level of competency in IPC standard protocols, showing very high competence in hand hygiene and in the use of personal protective equipment, and adequate competence in the prevention of needlestick and sharp injuries.
Inferential analysis further indicates that age and sex are not significantly related to nurses’ competency levels in IPC standard protocols, whereas professional variables such as educational attainment, clinical area of assignment, length of service, and attendance in relevant trainings, shows significant relationship with competency. In response to the identified gaps, particularly in consistent hand hygiene practices, specialized PPE utilization, and advanced sharpsinjury prevention, a training program titled “Enhancing Infection Prevention and Control Competencies among Emergency and Operating Room Nurses in the 5th District of Camarines Sur” is proposed as a targeted intervention to strengthen occupational safety and promote highquality patient care.
Recommendations
In light of the findings and conclusions, it is recommended that hospital administrators and nursing service directors prioritize structured capacity-building initiatives in infection prevention and control (IPC), particularly for the predominantly young, early-career nursing workforce with limited formal IPC training. This may include regular in-house seminars and workshops, supported by institutional measures such as flexible scheduling and funding assistance, to facilitate participation in external courses and conventions offered by organizations like the Department of Health and PHICS. Strengthening the culture of continuous professional development in IPC will help ensure that both foundational and advanced competencies are systematically reinforced.
Given that competency levels are generally high but comparatively lower in the prevention of needle stick and sharp injuries, unit supervisors may implement periodic safety audits, targeted skills drills, and scenario-based simulations focusing on sharps handling and occupational safety. These efforts can be complemented by continuous monitoring, constructive feedback, and positive reinforcement to sustain excellent practices in hand hygiene and PPE utilization while closing remaining behavioral gaps in sharps-related safety. Furthermore, because professional variables such as educational attainment, area of assignment, length of service, and prior training significantly influence competency, nursing management may integrate these factors into staffing patterns, mentorship arrangements, and preceptorship programs. Novice nurses can be systematically paired with more experienced and highly educated preceptors, while the proposed training program, “Enhancing Infection Prevention and Control Competencies among Emergency and Operating Room Nurses in the 5th District of Camarines Sur,” may be formally adopted, regularly evaluated, and continuously refined based on staff feedback and clinical outcome indicators to sustain both occupational safety and high-quality patient care.
References
- Abanes, L. & Villanueva, P. M. (2022). Infection Prevention and Control Practices Among Healthcare Providers in Level I Hospitals in Rinconada. Polaris Global Journal of Scholarly Research and Trends, 1(4), 134–146. DOI ↗ Google Scholar ↗
- Aguilar, R. (2023). “knowledge and practice of universal precaution in preventing nosocomial infections among nurses,” Journal of Environmental and Public Health (Volume 71, No. 13), 66-74. Google Scholar ↗
- Akinwaare, M.O. (2022). “Perceived barriers, knowledge and reported practices of infection control among clinical nursing and medical students of a Nigerian University,” International Journal on Infection Control (Volume 60, No. 12), 103-109. Google Scholar ↗
- Alam & Mahbub (2024). “Nurses’ knowledge regarding infection control at national institute of diseases of the chest and Hospital, Dhaka, Bangladesh,” International Journal of Advance Research in Nursing (Volume 52, No. 11), 39-46. Google Scholar ↗
- Alsaadi, Ismael Mohammed and Elfeshawy, Reda (2024). “Nurse’s Knowledge Regarding Prevention of Post-Operative Surgical Site Infection at AL-Hilla Teaching Hospital,” (Unpublished Doctoral Dissertation, Al-Mustaqbal University, 51001 Hillah, Babil, Iraq). Google Scholar ↗
- Alshamrani, M. M., Tannous, E., Othman, F., Al Zunitan, M., Abalkhail, M., & El-Saed, A. (2024). Competency level and determinants among infection prevention and control staff in the Middle East and North Africa region. BMC public health, 24(1), 2224. DOI ↗ Google Scholar ↗
- Asfaw, Nini (2023). “Knowledge and practice of nurses towards prevention of hospital acquired infections and its associated factors,”International Journal of Africa Nursing Sciences (Volume 51, No. 9), 94-99. Google Scholar ↗
- Bika, N. (2022). Operating room nurse job description. Workable. https://resources.workable.com/operating-room-nurse-job-description Google Scholar ↗
- Briones, J. (2022). “Your role in infection prevention,” Philippine Journal of Advanced Nursing (Volume 55, No. 10), 92-96. Google Scholar ↗
- Campo, L. K. C., & Remon, A. R. (2025). Knowledge and Practices of Nurses on the Prevention and Control of Healthcare-acquired Infections in a Private Tertiary Hospital in Baguio City. Acta medica Philippina, 59(3), 92–103. DOI ↗ Google Scholar ↗
- Centers for Disease Control and Prevention. (2024). Healthcare-associated infections (HAIs). U.S. Department of Health & Human Services. https://www.cdc.gov/healthcare-associated-infections/index.html Google Scholar ↗
- Chen N, Li S, Kuang Z, Gong T, Zhou W, Wang Y. (2024) Identifying a competency improvement strategy for infection prevention and control professionals: a rapid systematic review and cluster analysis. Health Care Sci.;3:53–66. DOI ↗ Google Scholar ↗
- de Claro, V., Bautista, N., Torralba, M. R., Castro, V. V., Lucero, M. A., Molleno, L. J., & Stan, L. (2023). Infection Prevention and Control in Public Hospitals and COVID-19 Temporary Treatment and Monitoring Facilities in the Philippines: Results of a Baseline Survey. COVID, 3(3), 336-347. DOI ↗ Google Scholar ↗
- Department of Health. (2022). Administrative Order No. 2022-0051: Revised National Policy on Infection Prevention and Control in All Public and Private Health Facilities. https://sites.google.com/view/doh-hfdb/updates/ao-2022-0051 Google Scholar ↗
- Desta, M. et.al. (2023). “Knowledge, practice and associated factors of infection prevention among healthcare workers,” Canadian Journal of Infection Control (Volume 37, No. 9). 13-17. Google Scholar ↗
- Diaz, C. (2022). “Nurses’ knowledge, skills and personal attributes for providing competent health education practice, and its influencing factors: A cross-sectional study,” Nurse Education in Practice (Volume 12, No. 2), 28-35. Google Scholar ↗
- Eberhard, D. M., Simons, G. F., & Robinson, A. J. (Eds.). (2026). Bikol, Rinconada. In Ethnologue: Languages of the world (29th ed.). SIL Global. https://www.ethnologue.com/language/bto/ Google Scholar ↗
- Ellasus, Jerome L. and Lopez, Freda B. (2023). “Infectious Diseases Prevention and Control Practices Among Healthcare Personnel,” (Unpublished Master’s Thesis, Urdaneta City University, Philippines). Google Scholar ↗
- Escalante, I. B. E., & Alcala, E. E. (2026). Infection prevention and control compliance among healthcare workers in rural district hospitals in the Philippines: A cross-sectional study. United International Journal for Research & Technology, 7(5), 60–70. Google Scholar ↗
- Gholizadeh, Leila (2023). “Effectiveness of implementing of an infection control link nurse program to improve compliance with standard precautions and hand hygiene among nurses: a quasi-experimental study,” BioMed Research International (Volume 58, No. 12), 65-72. Google Scholar ↗
- Grimm, C., Scheithauer, S., Artelt, T., Stieber, A., Erlenwein, J., Schuster, M., Bauer, M., & Waeschle, R. M. (2024). Evaluation of the practice of reprocessing ORs in German hospitals from an infection prevention and control perspective. Infection, 52(4), 1575–1584. DOI ↗ Google Scholar ↗
- Healthdirect Australia. (2024). Needlestick injuries. https://www.healthdirect.gov.au/needlestick-injuries Google Scholar ↗
- Hernandez, D. (2022). “Assessment of staff knowledge and practices for nosocomial infection control and prevention,” Health Education and Health Promotion (Volume 12, No. 1):159-164. Google Scholar ↗
- Hyeon, Y. H., & Moon, K. J. (2024). Development of an infection control competency scale for clinical nurses: an instrument design study. BMC nursing, 23(1), 250. DOI ↗ Google Scholar ↗
- Junejo, Zafarullah (2024). “Knowledge and Practice of Infection Control among Nurses at Liaquat Institute of Medical & Health Sciences Hospital, Thatta,” (Unpublished Master’s Thesis, Liaquat University of Medical and Health Sciences, Jamshoro, Pakistan). Google Scholar ↗
- Kilpatrick, M. (2024). Environmental theory of Florence Nightingale. Washington State Nurses Association. https://www.wsna.org/news/2024/environmental-theory-of-florence-nightingale Google Scholar ↗
- Kim, E. J., & Kang, J. (2025). Infection control nursing competency model for nurses in intensive care units: A Delphi study. American journal of infection control, 53(2), 203–209. DOI ↗ Google Scholar ↗
- Lamichhane G. (2025). Shaping professional nursing practice using Benner's novice to expert theory. British journal of nursing (Mark Allen Publishing), 34(22), 1133–1137. DOI ↗ Google Scholar ↗
- Luzon, W. M., Barlizo, A. L., Abaño, R. C., Andalis, M. R., Olea, J. N., & Martirez, B. F. (2025). Compliance level among healthcare workers of rural health units on the standard infection prevention and control. International Journal of Research and Innovation in Social Science, 9(10), 5969–6005. DOI ↗ Google Scholar ↗
- Macabangon, R., Abarquez, V. M., Usman, N., & Alipio, M. (2026). Occupational nosocomial infections among healthcare workers in a Philippine private hospital: Incidence and infection-prevention risk factors. International Journal of Transformative Multidisciplinary Studies, 2(1), 9–19. HAL Id: hal-05367070 Google Scholar ↗
- Makarawate, P., Garaygordobil, D. A., Carmona-Luna, T., Pruksamonthol, P., & van der Laan, A. D. S. (2026). Impact of structured adherence training on healthcare professionals: a pilot study in Mexico and Thailand. Frontiers in medicine, 13, 1758459. DOI ↗ Google Scholar ↗
- Merilles, L. (2024). “Guidelines for prevention of hospital acquired infections,” Philippine Journal of Critical Care Medicine (Volume 18, No. 3), 149-163. Google Scholar ↗
- Mrayyan, M. T., Abunab, H. Y., Abu Khait, A., Rababa, M. J., Al-Rawashdeh, S., Algunmeeyn, A., & Abu Saraya, A. (2023). Competency in nursing practice: a concept analysis. BMJ open, 13(6), e067352. DOI ↗ Google Scholar ↗
- Nalica, G. V. (2025). Level of Compliance of Staff Nurses in Infection Control Practices in Selected Hospitals in Puerto Princesa City, Philippines. Asian Journal of Research in Nursing and Health, 8(1), 793–803. DOI ↗ Google Scholar ↗
- NHS England. (2024). Chapter 1: Standard infection control precautions (SICPs). National Infection Prevention and Control Manual for England. https://www.england.nhs.uk/national-infection-prevention-and-control-manual-nipcm-for-england/chapter-1-standard-infection-control-precautions-sicps/ Google Scholar ↗
- Ocampo, Lyanne Kae C. (2024). “Knowledge and Practices of Nurses on the Prevention and Control of Healthcare-acquired Infections in a Private Tertiary Hospital in Baguio City,” (Unpublished Doctoral Dissertation, Saint Louis University, Baguio City, Philippines). Google Scholar ↗
- Palarpalar, Lorna A. (2023). “The interrelationship of the levels of knowledge, attitude and practices on infection control and selected demographic characteristics among hospital nurses in Dumaguete City,” International Journal of Nursing Studies (Volume 93, No. 17), 1114-118. Google Scholar ↗
- Qureshi, M. O., Chughtai, A. A., & Seale, H. (2022). Recommendations related to occupational infection prevention and control training to protect healthcare workers from infectious diseases: A scoping review of infection prevention and control guidelines. BMC Health Services Research, 22(1), Article 272. DOI ↗ Google Scholar ↗
- Rai, Kriti and Shakya, Shraddha (2022). “Knowledge and Practice regarding Infection Control among Nurses in a Private Hospital of Lalitpur,” International Journal of Community Medicine and Public Health (Volume 62, No. 8), 53-59. Google Scholar ↗
- Republic of the Philippines. (2019). Republic Act No. 11223: Universal Health Care Act. https://lawphil.net/statutes/repacts/ra2019/ra_11223_2019.html Google Scholar ↗
- Sangkula, Sahid (2024). “Nurses' Compliance Towards Infection Control Practices at Sulu Sanitarium and General Hospital,” Philippine Journal of Interdisciplinary Perspectives (Volume 21, No. 6), 47-53. Google Scholar ↗
- Shaban RZ, Macbeth D, Considine J, O’Sullivan M, Collignon P, Mitchell BG, et al. (2025) Protocol to establish standards for the elements of infection prevention and control programs and practice and competency standards for infection control professionals in Australian hospitals. PLoS One 20(8): e0330221. DOI ↗ Google Scholar ↗
- Shrestha, G.N. and Thapa, B. (2023). “Knowledge and practice on infection prevention among nurses of Bir Hospital, Kathmandu,” Nepal Health Research Journal (Volume 81, No. 16), 77-83. Google Scholar ↗
- Tamoor, Iqbal, Bisma, Fater B. and Sajid, Ali (2024). “Knowledge, Attitude and Practice of Nurses Regarding Infection Control in Operation Theater in Secondary Care Hospital,” Menoufia Medical Journal (Volume 37, No. 6), 58-64. Google Scholar ↗
- Toney-Butler TJ, Gasner A, Carver N. Hand Hygiene. [Updated 2023 Jul 31]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2026 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470254/ Google Scholar ↗
- United Nations. (2026). The 17 Goals. Sustainable Development. https://sdgs.un.org/goals Google Scholar ↗
- Webb, A. (2024). PPE: Definition, meaning, gear, and equipment. MCR Safety. https://www.mcrsafety.com/blog/ppe Google Scholar ↗
- Western Governors University. (2026). ER nurse career. https://www.wgu.edu/career-guide/healthcare/er-nurse-career.html Google Scholar ↗
- World Health Organization. (2026). Infection prevention and control. https://www.who.int/health-topics/infection-prevention-and-control#tab=tab_1 Google Scholar ↗
- Yousaf & Tahira (2022). “Nurses Knowledge and Attitude Regarding Infection Control Practices,” Journal of Health and Rehabilitation Research (Volume 48, No. 10), 78-84. Google Scholar ↗